Recently we’ve been revisiting our thinking around an organisational data strategy. For me, this means getting some sound principles discussed and agreed. A first pass at writing some ideas down feels a bit more like a data manifesto but (I think) gives a possible starting point.
As a disclaimer, while I refer to my organisation, the Northern Care Alliance (or NCA) what follows are initial, personal thoughts only.
Really interested in anyone’s feedback or views.
@chorltonjim
Draft data manifesto
Principles
The NCA aims to be a data driven organisation. Therefore our approach to data acquisition will require senior focus to catalogue
- measurements where a universally accepted definition can be communicated. Where definitions cannot be agreed, data will not be reported
- controllable & influenceable input metrics that the organisation believes drive critical output measures. Data driven management will focus on improving these input measures.
- output measures of value. These will be tracked but will not be the driver of data driven management. It is accepted that some measures could function as output metrics for one area and input metrics for another area. In these cases, the NCA will focus on the ‘root cause’ and align on downstream input metrics.
E.g. out of hours critical care step downs will be considered an output measure. Instead of tracking this, focus would be given to measuring times of clinical decision making re: suitability for ICU discharge, time taken to communicate this with bed management teams…
Critically, the NCA recognises that it is impossible to manage a complex adaptive system solely through the use of data. Organisational feedback loops will be required to feed up to executive level to identify areas where staff or patient stories are mis-aligned with reported data. The value of these narratives will never be overlooked.
The NCA will value data in the same way they would a capital asset. Based on estimates from data breaches on their resale value, complete patient records are valued at up to $250. The NCA will validate their own value estimates of data assets and use this to support the case for investment in the creation and curation of these assets.
Further to this, the NCA will aim to maximise the long term value of the data assets it creates by focussing on data completeness, cleanliness and standardisation. Achieving this will require executive support to promote consistency in data capture at the price of reduced flexibility in data capture until the data driven culture becomes self sustaining. The risk to organisational engagement from this approach will be mitigated through the understanding of the value of the data asset being created – this information will be used to create incentive structures to reward the work provided in data creation.
It is accepted that different classes of data will have differential values (and that these may vary depending on whether presented to an internal or external audience). As part of the business planning cycle and research and innovation strategy, the NCA will actively manage a process to track and manage a hierarchy of data value. This will allow incentives for data collection to be appropriately targeted.
As a public organisation, the NCA will commit to publicly sharing data quality and data capture metrics. This will enable the organisation to be held to account, will promote external peer review, and will drive discussion regarding the best measurements e.g. year on year improvement vs. Absolute descriptions.
The NCA will operate under the working assumption that patients have an inalienable right to access their own healthcare data. We will
- work with patient groups to define an optimal Personal Health Record and data sharing strategy
- actively promote the role of the patient in the creation and curation of their own data
At the defined point in the lifecycle of data assets, the NCA will move to recognise these as a public rather than organisational asset. At this point, in a manner compliant with contemporaneous information governance legislation, data will be made publicly available with the only requirement for users being recognition of the NCA and its patients in the creation of this asset.
Data as an exponential opportunity
Opportunities for exponential growth and value creation occur when technologies and markets converge around the same opportunity. This is occurring for healthcare data.
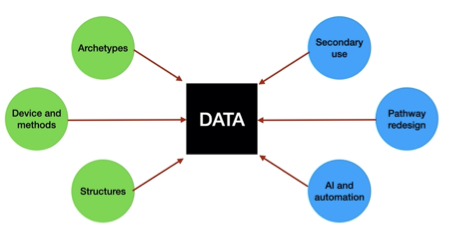
Technical convergence is happening through
- improved data archetypes and meta-models
- better tools to enable data capture
- agreement on data standards for collection, storage and messaging
Market convergence is represented through
- secondary use of data for research and innovation
- pathway redesign in the emerging ICS model
- tools to use AI and automation to release value form data
To realise this opportunity, the NCA will track key enablers of technical exponential growth:
- digitalisation; we will commit to all data being digital unless there is a critical reason to not do
- deception; the NCA will develop in house market awareness to understand when technologies are between hype and reality
- disruption; although impossible to predict at this point what organisational changes will be created by transforming into a data driven organisation, the NCA accepts a priori that there will be a need to rapidly adapt to new ways of work that will be created through intelligent use of data
- demonetisation by working with expert finance and procurement colleagues we will develop ways to efficiently model reducing long term costs of data and technology storage & acquisition. This mandates an acceptance that costs may be front weighted.
- dematerialisation; the NCA will embrace the opportunity in data and technology to reduce the need for physical products and estates e.g. data driven improved models of care may reduce the physical footprint of our estate
- democratisation; the NCA will view ownership of data assets in a broad sense. Patients will be provided access to their own data; staff will be supported through self serve analytics and the wider population will be provided with long term access to openly published data sets.
Addressing risk
Nationally the ‘Data Saves Lives’ document provides a clear description of the safety value created through efficient and timely data sharing between organisations.
With the NCA we will mirror this with internal messaging that ‘Data Prevents Harm’. We will work with clinical and operational leads to understand elements of organisational risk that can be efficiently mitigated through data. This creates a trajectory for us to be both
- reactive with real time information on harm or potential harm, reducing time to response; and
- proactive using data to estimate risks at patient and population levels enabling harm reduction
This approach can be mirrored in support of targeted improvement activities. We will use data to track the opposite of the IHI triple aim – the triple fail to understand and adjust clinical scenarios where patients routinely have a poor experience with poor healthcare outcomes and high costs of care.
An example of a triple fail is unplanned harm-dialysis initiation. Here patients are admitted (at high cost); require urgent painful vascular access (poor experience); and have reduced life expectancy and likelihood of access to transplantation (poor outcome).
Long term vision
The NCA data strategy must lay the framework for future models of care, aligned to the NCA vision of person and place. Therefore delivery must facilitate a transition from an episodic, hospital centred model of care towards a continuous and distributed model. Achieving this will allow
- personal needs to be balanced with population management
- care to be delivered at the time and place of need
- multichannel delivery
Key to this is successful deployment of an open NCA digital architecture.
In tandem, there must be a recognition of the move towards greater consumerisation in healthcare. The NCA data strategy here must support patients in the choices they make in coordinating their care, through a willingness to share data (at the patient’s request and with appropriate information governance in place).
The NCA data lifecycle
The NCA data strategy must address all phases of a data lifecycle from creation to aggregation / storage and consumption to deletion. The data strategy will inform parts of the technology and device strategies, but must be robust to the individual staff needs. Time must be invested in structuring the collection of data to speed time to reuse i.e. reduce ETL timelines. This will support self service analytics and the delivery of the Research and Innovation Strategy.
The renal service has now established a multi-morbidity clinic which is unique in the NHS. Through Principle Investigator funds, data collection forms are being developed in EPR which provide a clinical record as their primary function, and offer a ‘live feed’ into a research quality database that is valuable to the service and to industry partners.